Category — Health research
What did you say?

If I work hard enough I can control any situation.
I am worthy as long as I am successful
When is the other shoe gonna drop?
No one understands me.
Ah yes, those voices inside our heads. Okay, my head. You too? Maybe not these voices but others? That voice that tells you have to be perfect. That voice that tells you to avoid conflict and therefore mask your feelings. That voice that tells you receiving help means being helpless.
Do not worry, my friends., I have not morphed into a spouter of self-help gobbledegook. I am not about to (gasp) write a book about any of this. The shelves are groaning with books like this.
But I am interested in this take on those sabotaging voices inside our heads by the “positive intelligence” training guru and, yes, best-selling author, Shirzad Chamine, a Stanford lecturer and Fortune 500 corporate coach. By the way, you might consider not buying his book. He does not need your money.
Speaking Fee:
Live Event Fee: $30,000 – $50,000
Virtual Event Fee: $10,000 – $20,000
But you can take his “Saboteur Assessment” test for free—and you might learn something about yourself. Or, like me, nod your head in agreement about what you already know about yourself. Because those (potentially) sabotaging voices are so very familiar.
Can I (we) just stop listening? I doubt it. (Oh no, is that one of my saboteurs talking to me?) I do think that by naming these voices—Charmine identifies 10—we can at least recognize what they are doing, or the dark and unproductive places they “illuminate” for us. And then…Reason with them? Shout them down? Stuff a sock in their mouth?
Here are the nasty little beings making noise inside your (my) head. Tell them to shut the fuck up. (That’s probably not the advice what Shirzad Charmine charges $50,000 for.) Mine is free!
- Judge
- Controller
- Hyper-achiever
- Restless
- Stickler
- Pleaser
- Hyper-vigilant
- Avoider
- Victim
- Hyper-rational
March 22, 2023 6 Comments
The happy writer. Really?

Can we write our way to happiness?
On first blush this question oozes self-indulgence and privilege. More woo-woo bullshit.
On second blush, “can we write our way to happiness?” could be the rhetorical tagline for those enticing writers’ workshops in Tuscany.
But there is actually a body of scientific research on the health and mood benefits of writing and rewriting one’s one narrative. (Google “expressive writing and health” for many citations.) There is significant research on story-crafting and behavior.
We all have a personal narrative that shapes our view of ourselves and the world(s) in which we live. We create that narrative. We construct stories out of experience. We listen to others tell us about ourselves. We learn–even if we don’t think we are learning, even if we don’t want to– what is expected, what is acceptable, and how we fit (do not fit) in. Over time, a grand narrative emerges. And we recite it to ourselves. Over and over. We believe it. We inhabit it. For some, this can be harmful, limiting, even debilitating.
What if we wrote it out this story. Looked at it. And then learned to tell another plausible tale, an alternative narrative, based on the same information.
That’s what researchers at Duke University did with a group of freshmen who (because of bad grades) told themselves they were losers, that they were unfit for college. That was their narrative. These students underwent a “story-changing intervention” during which they got information (and were exposed to inspirational videos) about students who struggled during freshman year but improved as they adjusted to college. The “loser freshman” story could then be recast into an upward trajectory, “this is just all part of growth and adjustment” story. And guess what? Students who had been prompted to change their personal stories improved their grades and were far less likely to drop out than the control group with no intervention.
I thought about the notion of writing one’s way to a more positive self-image, a healing place, an invigorating place, a place of power and self-worth every time I sat with my writing group at Oregon State Penitentiary. They were all serving life sentences for murder. To move beyond debilitating shame and endless guilt, they wrote about the men they were learning to become, the men they had become. They were changing the narrative of their lives.
I think about the woman in my recent university seminar, emotionally brutalized at one of those “bad teen” bootcamps, who is, more than a very tough decade later, writing her way to stability and health. I think about the women in the workshops I am now teaching who use writing as a way to process the pain they have tried so long to ignore.
It is talk therapy when you do the talking. It works.
March 15, 2023 3 Comments
Performative Compliance…whaaat?

I’m going to coin a new phrase here. At least I have not come across it elsewhere: Performative Compliance.
This refers to the actions of states, cities, businesses, schools in the face of the persistent threat of COVID-19. I’ve been thinking about this since I temporarily left my Eugene Bubble and ventured out into one of those states that is not, to put it mildly, part of the “blue sweep” many of us are hoping (and working) for 13 days from now.
I think there may be 3 levels of compliance to those protocols SHOWN and PROVEN to mitigate the spread of the virus.
First is true adherence. Every public indoor place has a “no admittance without a mask” sign prominently displayed. And THERE IS NO ADMITTANCE WITHOUT A MASK. As in, enforced. Public indoor places have FLOOR MARKINGS to help people stay at least 6 feet apart from each other. Other spaces are reconfigured to make this possible. GLOVES and hand sanitizer are everywhere. In restaurants (with indoor or outdoor seating), there are no ketchup bottles, salt and pepper shakers on the table, nothing that would be touched by many people. And much more.
The second is what I have discovered in my out-of-the-bubble experience: Performative Adherence. I’ll just give this one example. On one end of a table is an ice/ water dispensing machine operated by 2 touch buttons. Two feet away, on the other end of this table, taped to the table itself (so not at eye level) is a sign that says you should wipe down high-touch surfaces. The wipes are not there. The wipes are in an unmarked plastic container on a shelf located elsewhere. Did anyone who used the ice machine see the sign, find the wipes and obey? I stood to the side and watched 4 people. No one saw the sign. Each person touched the button the previous person had touched.
Did the facility comply to the “wipe surfaces” mandate? You be the judge.
The third level, which I have not experienced but, like all of you, have read about in social media, or seen in videos featuring parades of the maskless marching through big box stores, is no compliance at all. These are folks who call COVID the “Wu-Han virus” and believe the ongoing pandemic is mostly a figment of the Left’s imagination. Their interpretation of our President’s recent bout of illness is: See, it’s not that dangerous. Or: What a dude! How strong! How invincible!
It’s Level 2 that I find so disturbing. Entities pretending to obey mandates and policies but making it easy for no one to obey. Doing what you have to do to avoid litigation but not what you are supposed to do to avoid creating an unhealthy environment. It’s the sneakiness of it, the backhandedness of it. At least the maskless mobs are “true” to their beliefs.
October 21, 2020 6 Comments
America’s status in the world

On the occasion of Bloomberg Health Index’s announcement of the healthiest countries of 2020…take a wild guess at the US’s ranking…(or, you cheater, skip to the end and see) added to the President’s incessant, incoherent, hallucinatory ramblings about how great we are, I feel compelled to ask:
Just how great are we? What exactly does the US rank #1 in?
We lead the world in:
...COVID cases. We are 5 percent of the world’s population and have 30 percent of the confirmed cases.
…the cost of health care. Ours is the most expensive in the world.
…the incarceration of men and women. By pure number. By percent of population. By any way you can count it.
…our military spending.
Here are #1 ranking in other areas that might interest you:
#1 Most innovative: Switzerland
#1 Most technologically advanced: Japan
#1 in use of renewable energy: Sweden
#1 Cleanest environment: Finland
#1 Highest worker productivity: Germany
#1 Highest median family income: Norway
#1 Healthiest: Spain
#1 Safest: Singapore
#1 Lowest Infant mortality: Luxembourg
#1 Best healthcare system: Luxembourg
#1 Longest life expectancy: Monaco
#1 Most educated: Singapore
#1 Highest literacy rate (100%) Andorra, Luxembourg, Greenland, Norway
#1 Narrowest gender gap: Iceland
#1 Most LGBGTQ-friendly: The Netherlands
#1 Happiest: Norway
Now to the Bloomberg Index. Each year statisticians pour over country-by-country data on pollution, water quality, access to health care, health risks in the population (smoking, obesity, high blood pressure), malnutrition, life expectancy, causes of death. Taking these and other factors into account, the Index ranks 169 countries. The top (healthy) score is 100. (The data are pre-pandemic.)
This year Spain (92.75) placed first, edging out last year’s first-place Italy. Here are the top 10:
- Spain
- Italy
- Iceland
- Japan
- Switzerland
- Sweden
- Australia
- Singapore
- Norway
- Israel
Where, oh where, is the US in this ranking? We are #35.
Among those countries ranked healthier than us: Cuba, Croatia, Estonia, Chile, Slovenia. (And, of course, the unsurprising ones: Canada, UK, New Zealand, Germany, France, Austria.)
Our greatness at this moment can be our recognition of our faults and our embrace of meaningful and compassionate change. It is this thought that allows me to sleep at night.
June 24, 2020 2 Comments
A virus has no politics
One of the more repulsive and terrifying things about this pandemic is how quickly it was cast (and is being played out) as a political issue.
A virus has no politics.
The decision to stay at home, to mask up when attending to essential business is not political.
The medical researchers in labs around the world working on potential vaccines are not compelled by whatever their personal political beliefs might be.
The nurses and doctors putting their own health at great risk to care for others are not compelled to do so based on whatever their personal political beliefs might be.
Yet the man who–to our great shame—is currently our president has made it into a political issue. This is not just (as so much of what he does and says and is) reprehensible. It is dangerous.
I gasp at his off-the-rails televised public briefings, at his ongoing “leadership” of the right-wing’s devaluation and dismissal of science, at the bizarre alt-right conspiracy theories concerning the origin of the disease, at the “patriot” zealots calling for taking to the streets to re-open businesses because government closures violate our constitutional rights. At preachers, spouting political rhetoric, who tell their flocks to gather en masse because god will protect the righteous.
There is no room for posturing here. Or grandstanding. Or twitter-ranting. COVID-19 and what we do now–the careful, informed, compassionate apolitical choices we make to save lives and help our communities recover–will define our humanity. The man who–to our great shame–sits in the White House has shown, in this crisis, what kind of a human he is.
We need to listen to real leaders. Like the governors of Oregon, Washington and California who issued this joint statement about planning our “comeback”:
“Health outcomes and science – not politics – will guide these decisions. Modifications to our states’ stay at home orders must be made based on our understanding of the total health impacts of COVID-19, including: the direct impact of the disease on our communities; the health impact of measures introduced to control the spread in communities—particularly felt by those already experiencing social disadvantage prior to COVID-19; and our health care systems’ ability to ensure care for those who may become sick with COVID-19 and other conditions. This effort will be guided by data. We need to see a decline in the rate of spread of the virus before large-scale reopening, and we will be working in coordination to identify the best metrics to guide this.
Public health experts like Dr. Fauci urge extreme caution about resuming normal life too soon for fear of instigating another wave of illness and death.
When to “re-open for business” is NOT a political decision.
April 15, 2020 4 Comments
Prisons and COVID-19

This morning began with the distressing—but completely expected—news of the first confirmed case of corona virus at an Oregon prison. The person is an employee at Oregon State Penitentiary in Salem, the state’s only max, where more than 2000 men live—most doubled-up in cells meant for one person, cells the size of your bathroom. This is the prison I know well, having spent more than four years as a volunteer there running a writers’ group for Lifers. I went in and out of that prison close to 100 times. I was there early last month visiting an inmate. Two days later, in response to the virus threat, the Department of Corrections closed all the prisons and jails in the state to visitors.
That was a smart move. However, as everyone familiar with this prison knows, OSP houses the state’s second largest commercial laundry, which receives thousands of tons of dirty linen from state hospitals and other institutions. It is unclear what precautions, if any, were taken in response to the threat.
But the virus entered the prison through an employee. With more than 4,500 people working for the Department of Corrections, many hundreds of them staffing three shifts at OSP, the virus has had so many opportunities to enter that it is surprising it took this long. The place is on lockdown as of this morning. That means everyone is confined to their cell 24/7 (except…if this lockdown is like the others…those inmates who work for the laundry).
In a letter to the director of the Department of Corrections, Colette Peters, officials with ACLU Oregon, the Oregon Justice Resource Center, Oregon Criminal Defense Lawyers Association, Partnership for Safety & Justice and Sponsors, Inc., asked her to reduce the prison population by considering people for early release.
“Given the mortality rate associated with the virus, we are concerned about the virus’s spread to at-risk people, particularly the elderly, within the closed confines of a prison setting,” they said in the letter. (Please see ACTION item at the bottom of this post.)
A 2012 study by the ACLU found that Oregon had the ninth-largest population of senior-aged prisoners in the United States, despite being only the 27th largest state by population. Research also shows that people in prison have higher rates of “co-morbidities,” those conditions (diabetes, heart disease, asthma) that make a person more vulnerable to the virus and far more likely to die from it.
If you have been tracking news about the virus and prisons, you know that Cook County Jail (Chicago) has recently reported at least 113 cases involving both inmates and staff. In the federal system, at least 52 inmates and prison workers across the U.S. have tested positive, including a cluster at the federal prison in Atlanta.
A worker there (speaking on condition of anonymity, fearing retaliation) made this point: “We do not have enough masks; we do not have the supplies needed to deal with this. We don’t have enough space to properly quarantine inmates.”
This would be true across ALL prisons and jails. These places where we warehouse 2.3 million people are, in the words of epidemiologists tracking the pandemic, “petri dishes.”
PROTECT OREGON INMATES FROM CORONAVIRUS (COVID19)
Please email, call, Tweet, mail
Governor Kate Brown:
Twitter @OregonGovBrown
900 Court Street, Suite 254, Salem, OR 97301, Phone: 503-378-4582
April 1, 2020 4 Comments
It IS broke. Let’s fix it.

I’ve spent more time inside a prison than most civilians. And I’ve probably spent more time reading about and thinking about incarceration than most people who don’t study or work for the corrections industry.
I know, as much as a civilian can know, what that environment feels like. It is soul-crushing. Much has been written about the damage incarceration inflicts—from teaching helplessness to sparking hostility, from exacerbating mental health issues to eroding the physical and emotional health of the children of the incarcerated. And much has been written about the system’s failure to do what we want it to do: reduce crime.
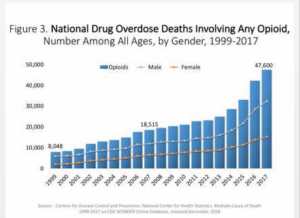
But until I read this study in Lancet (0ne of the oldest, most prestigious science journals),
I had not considered that our epidemic of mass incarceration might be linked to the astonishing rise in drug overdose fatalities we’ve all been reading about.
Yes, it’s not news that prison and drugs are linked. The war on drugs accompanied by tough-on-crime mandatory sentencing policies sent and continues to send hundreds of thousands to prison. And yes, a significant percentage of people who commit crimes have some involvement with drugs. (Women’s crimes, in particular, are often to support drug habits.) And yes, drugs are a problem inside prison.
But this study in Lancet suggests an entirely different connection between incarceration and drugs. Based on meticulous crunching of several huge data sets, the study concludes that there is a strong association—a “robust connection”– between the rise in incarceration rates and deaths from drug use.
Data came from 2,600 counties across the country and spanned 1983-2014. The study found that, on average, counties with the highest incarceration rates saw a drug mortality rate 54 percent higher than the rate among counties with the lowest incarceration rates. (The relative poverty of the community accounted for half of this difference; the other half was the rate of incarceration.)
Incarceration, they write, “is directly associated with stigma, discrimination, poor mental health, and chronic economic hardship, all of which are linked to drug use disorders.”
Here’s how one of the co-authors of the study, an economics professor at University of Massachusetts, put it: “In communities with high incarceration rates, it’s making their lives much worse, and making them much more likely to use drugs dangerously.”
In other words, if you came to prison with a drug problem (as a reported 50 percent do), then when you are released (as 95 percent of prisoners are), the conditions are ripe for continued or increased abuse. If you didn’t already have a drug problem, the experience of and stigma attached to incarceration might pave the way to abuse.
July 10, 2019 1 Comment
Test me! Treat me!

I am about to go off to the dentist for a routine hygiene/ cleaning appointment where, once again, I will be told I need a new set of x-rays, and once again, I will decline. I take good care of my teeth, see my hygienist three times a year, have no problems/ symptoms, and submit to x-rays every 3 years or so. That is ENOUGH.
I was thinking about this “testing for everything because we can” approach to medicine after reading Barbara Ehrenreich’s bold essay on “Why I’m giving up on preventative care.” She goes too far for me. I don’t see a colonoscopy as rape-by-machine, and frankly I’d rather have an innocent polyp removed than hang around waiting for it to maybe become something. And her point about testing and treating to prolong life doesn’t resonate with me. I am not interested in prolonging life. I am interested in prolonging good health. (Those of you who’ve heard me speaking about this or have read my book, Counterclockwise, know my favorite geeky term for this: rectangularization of morbidity.)
But Ehrenreich makes many good points in this essay. As testing gets more and more sophisticated, the chances for finding something increase. Whether than something is worth worrying about (let alone aggressively treating) is another matter.
This relates to two other health and medicine issues I’ve been contemplating, the value-added component of living with a science writer.
The medicalization of our lives. In above-mentioned science writer Tom Hager’s words (from his upcoming book chronicling 10 drugs that changed our world) this is “a troubling trend in our society, in which things that we once simply dealt with on our own – like lifestyle choices, low-risk health conditions, personality quirks – are now being turned into treatable medical conditions. Often this goes hand-in-hand with the appearance of a new drug suited to treating the new condition.” Everyday anxiety, for example. Classroom misbehavior. Or, gee, how about menopause?
Disease mongering. This is emphasizing or redefining the risks of disease to enlarge the market for medications. For example, even though medical researchers have known for many many years that the total cholesterol number is meaningless, that “number you should be scared about” has gotten lower and lower. When just about everyone is at risk, that means everyone should be treated preventively, right? As Tom Hager writes: “Minor problems can become major money-makers for drug companies. With a much larger group of potential patients getting increasingly worried about their risks, the market for the drug grows. Blockbusters can result.” Cholesterol-reducing statins are blockbusters.
Now we have entered into the world of sophisticated mail-in genetic testing, where I can discover (if I want to) all the disease demons lurking in my DNA. Oh boy. I think I’ll just eat an apple and go for a run.
April 18, 2018 4 Comments
Writing your way to happiness

Can we write our way to happiness?
On first blush this question oozes self-indulgence and privilege. More woo-woo bullshit. An unwelcome resurrection of the Me Decade. (Forgive the reference, now impossibly quaint, as we suffer under the “leadership” of GNOTUS…Grand Narcissist of the United States.)
On second blush,“can we write our way to happiness?” could be the tagline for endless Writers’ Workshops in Tuscany.
But stay with me for a moment. There is a body of actual scientific research (remember what that is?) on the health and mood benefits of writing and rewriting one’s one narrative. (Google “expressive writing and health” for many citations.) Now there is research on story-crafting and behavior.
We all have a personal narrative that shapes our view of ourselves and the world(s) in which we live. We create that narrative. We construct stories out of experience, listen to others tell us about ourselves, learn (even if we don’t think we are, even if we don’t want to) what is expected, what is acceptable, and how we fit (do not fit) in. Over time, a grand narrative emerges. And we recite it to ourselves. Over and over. For some, this self-talk is debilitating.
What if we wrote it out this story. Looked at it. And then learned to tell another plausible tale, an alternative narrative, based on the same information.
That’s what researchers at Duke University did with a group of freshmen who (because of bad grades) told themselves they were losers, that they were unfit for college. That was their narrative. These students underwent a “story-changing intervention” (oh, I know, shades of 1984). But wait…in this intervention, they got information (and were exposed to inspirational videos) about students who struggled during freshman year but improved as they adjusted to college. The “loser freshman” story could then be recast into an upward trajectory, “this is just all part of growth and adjustment” story. And guess what? Students who had been prompted to change their personal stories improved their grades and were far less likely to drop out than the control group with no intervention.
I think about the notion of writing one’s way to a more positive self-image, a healing place, an invigorating place, a place of power and self-worth every time I sit with my writing group at Oregon State Penitentiary. They are all men serving life sentences for murder. Collectively, they have spent more than two centuries behind bars. There are eight of them. Do the math. To stay sane, to move beyond debilitating shame and endless guilt, they write about the lives they now live, the men they are learning to become, the men they have become. They are changing the narrative of their lives.
April 11, 2018 2 Comments
Wanna hear me vent?
 I just need to vent, you say (I say) right before launching into a litany of complaints: the stupidity and gross incompetence of others, liars and hypocrites in government, how GBBS is shit without Mary Berry, the discovery of another varicose vein, the unfairness of the universe, et cetera et cetera and so forth.
I just need to vent, you say (I say) right before launching into a litany of complaints: the stupidity and gross incompetence of others, liars and hypocrites in government, how GBBS is shit without Mary Berry, the discovery of another varicose vein, the unfairness of the universe, et cetera et cetera and so forth.
Your friend listens. Then she vents.
And then you both feel better, yes?
And then you both feel better, no.
For those who still believe in science (uh oh, that was kind of a backhanded vent), let me explain. According to psychologists who have studied venting, not only does expressing negativity tend to make us feel worse, not better, it also makes listeners feel worse. Kind of like second-hand smoke.
So your mood worsens; your friend’s mood worsens – and, according to neuroscientists, your brain begins to wire itself for negativity.
You know how this works: Throughout your brain are little gaps between nerve cells (synapses). Chemical and electrical bridges are built between these synapses as you think, learn – and, yes, as you complain…that is, as you have recurring negative thoughts. The more often you think (and express) these thoughts, the stronger the electro-chemical bridge becomes. The brain is rewiring itself to make it easier and quicker to think these thoughts. It’s just being efficient. This means that not only do repeated negative thoughts make it easier to think yet more negative thoughts, they also make it more likely that negative thoughts will occur to you in other situations. A kind of default.
Also, the act of venting about something you’re upset about can, itself, make you upset. Reliving and narrating the anger (disappointment, frustration, whatever) you have felt can trigger the stress hormone cortisol. You know the demon, right? Not only does it inflict temporary harm (for example, raising blood pressure), excess cortisol over time leads to chronic inflammation. That’s the inside kind you can’t see or feel, the kind that medical researchers are beginning to believe underlies just about every chronic disease.
Venting makes you sick!
I am NOT suggesting suppressing anger. We all know that doesn’t work. I am suggesting going zero-to-sixty from pissed off to possible solution, from “this sucks” to “this is what I’m going to do about it,” from anger to action.
Now would be a really great time to get crackin on this.
June 21, 2017 5 Comments